Dr. D. Dutta Roy, Ph.D.(Psy.)
LECTURE NOTES ON SENSATION,ATTENTION AND PERCEPTION :PROBLEMS OF CONSCIOUSNESS
PERFORMING ART THERAPY CENTRE
RABINDRABHARATI UNIVERSITY
KOLKATA
12.1.2011
SENSATION
Sensation refers to awareness of stimulus. Stimulus refers to any thing that elicits response. This may be internal(changes in organ system) or external changes (changes in surroundings). There are five sensory organs excited by different types of stimuli.
1. Visual organ (Eye): Light
2. Auditory organ (Ear): Sound
3. Gustatory organ (Tongue):Chemical
4. Olfactory organ (Nose): Chemical
5. Cutaneous organ (Skin): Temperature,pressure
There is another organ named as kinesthetic organ excited by movement sensation. There are different attributes of sensation as
1. Quality: Generic quality (light and sound), specific quality (red, blue)
2. Quantity: Low and high frequency of sound
3. Localization: sensing pressure across different areas over skin
It will be misnomer to assume that any change in physical stimulus on physical scale causes same amount of change in the response scale. This is illustrated in problems of psychophysics. Psychophysics is a study to understand relation between changes in physical stimulus on physical scale and changes in response pattern on response scale. It discusses three types of thresholds of sensation as absolute, differential and terminal threshold.
Attention
When individual focuses awareness to something, attention takes place. Attention is focus of awareness. It has few functions like:
1. alerting: It is physical and mental preparedness to focus on specific stimulus.
2. selective function: Selectivity refers to a process by which attention is focused on stimulus or stimuli of ongoing interest and other stimuli are ignored.
3. limited capacity channel:limited capacity to carry out the task. We can process one task at a time. This causes serial processing.
4. vigilance: maintaining attention on a task continuously, for some
time, is called vigilance or sustained attention. It has been found that attending to a task for long is taxing, particularly if the task is monotonous and it leads to decrease in performance.
PERCEPTION
Perception occurs when sensation carries certain meaning. This can be explained in this formula:
Perception = sensation+meaning
Sensation = perception - meaning
visual perception must be viewed as an active process by which the visual information is interpreted and grouped according to a large number of rules. These Gestalt laws allow a phenomenological interpretation of the interactions between visual features that lead to the perception of composite objects. These laws are given below:
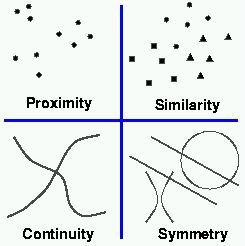
Laws of Perceptual Organization
(i) Good Form (Law of Pragnanz): This law states that perceptual organization will always be as “good” as the prevailing conditions allow. The simplest organization requiring the least cognitive effort will always emerge. Pragnanz means that we perceive the simplest organization that fits the stimulus pattern.

(ii) Proximity: All the stimuli that occur together in space or time will be organized together.

(iii) Similarity: Other things being equal, elements which are similar in structure or have common characteristics will be grouped together.

(iv) Closure: An incomplete figure will be seen as a complete one. a figure consisting of incomplete lines, that have gap in them. It is perceived as a triangle despite the fact that its sides are incomplete. A closure like phenomenon yields subjective contours.

AS ELEMENTS OF OUTER LAYER OF CONSCIOUSNESS
Success in performing art therapy depends upon its act on outer, inner and innercore layer of consciousness. The three layers of consciousness is given in Figure 1.

Figure 1 Layers of consciousness
Through performing art, one can start journey from outer to innercore layer through inner layer. Figure 2 shows the journey by Rabindrasangeet.
Faulty or poor development of outer layer inhibits this journey.

Figure 2 Rabindrasangeet is a journey across layers of consciousness.
Outer layer of consciousness concerns attention, sensation and perception. Any abnormality in these three causes serious problem in formation of inner and inner core layers of consciousness as these three play critical role in information processing model (Figure 3) specially in relation to filtering stimuli, retaining in memory stores and in developing imagery processes.

Figure 3. The Information Processing Model of Memory (Based on Atkinson and Shiffrin, 1968)
[Ref. Stevens Handbook of Experimental Psychology (2002) 3rd Edition, Volume 2: ‘Memory and Cognitive Processes’. John Wiley & Sons, Inc.; pp 10].
This multi store memory model is later expanded upon by Baddeley and other co-workers and has become the dominant view in the field of working memory (Figure 4).
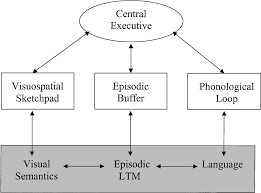
Figure 4 Baddley's working memory model
The original model of Baddeley & Hitch was composed of three main components; thecentral executive which acts as supervisory system and controls the flow of information from and to its slave systems: the phonological loop and the visuo-spatial sketchpad. The slave systems are short-term storage systems dedicated to a content domain (verbal and visuo-spatial, respectively). In 2000 Baddeley added a third slave system to his model, the episodic buffer. This component is a third slave system, dedicated to linking information across domains to form integrated units of visual, spatial, and verbal information with time sequencing (or chronological ordering), such as the memory of a story or a movie scene. The episodic buffer is also assumed to have links to long-term memory and semantical meaning.
ABNORMALITIES & PERFORMING ART THERAPY
Faulty development of outer layer creates mental illness due to inability to learn. Therefore, attention should be paid to these three processes in order to understand functional efficacy of the outer layer. ADHD or AD, Mentally challenged or mentally retarded children, HIV and Schizophrenic patients suffer from poor organizing functions of outer layer of consciousness.
ADHD or AD: Attention deficit hyperactivity disorder (ADHD or AD/HD or ADD) is a neurobehavioral developmental disorder. It is primarily characterized by "the co-existence of attentional problems and hyperactivity, with each behavior occurring infrequently alone" and symptoms starting before seven years of age. Function and outcome of Autism spectrum disorders (ASD) are affected not only by core deficits but by frequently associated comorbid behaviors- such as irritability, sensory abnormalities, hyperactivity, affective disorders and others. Outcome is further affected by the presence or absence of language and by overall cognitive ability. Robert Sears, M.D., discussed top 7 therapies for autism in his recently published book. To him, “Every child with autism is unique, and so each therapy program should be individualized to meet his or her needs,”. The 7 therapies are (i) Applied Behaviour Analysis (ABA), (ii) Relationship based floor-time therapy, (iii) Functional communication training, (iv) Language therapy, (v) Picture exchange communication system, (vi) Occupational therapy (viii) Treatment and Education of Autistic and Related Communication-Handicapped Children or TEACCH. In another experiment, it is noted that by using Rabindrik dance to one child diagnosed as autistic by NIMHANS., Bangalore, attentive behaviour is controlled. One performing art therapist was asked to train the child Rabindrik dance " Phule phule dhole dhole". The autistic boy initially could not attend to eye movement but he gradually followed each eye and posture movement of the therapist and finally was able to coordinate eye and posture movement keeping in tune of the music. This suggests that one can control outer layer of consciousness by performing art with patience and hierarchical structuring of the dance movement. In this experiment, therapist had used classical conditioning and patting, hugging, verbal reinforcements were the reinforcements.
Mentally challenged or Mentally retarded: In case of mentally challenged or mental retardation, problem is related to impaired cognitive functioning and deficits in adaptive behaviour. Usually their IQ and SQ are below 70 using standard intelligence test and adaptive behaviour test like Vineland Social Maturity scale. Below are the ranges of IQ and corresponding classification of mentally disorder.
Profound mental retardation: Below 20
Severe mental retardation: 20–34
Moderate mental retardation: 35–49
Mild mental retardation: 50–69
Borderline intellectual functioning: 70–84
To provide performing art therapy to mentally retarded children, it is important to follow different principles of behaviour modification technique like shaping, token economy etc.
HIV: Human immunodeficiency virus (HIV) infection is associated with an increased risk for human herpes viruses (HHVs) and their related diseases and they frequently cause disease deterioration and therapeutic failures. Cognitive impairments are one of the major consequences of HIV infection in the human body – as the virus, once in the blood stream, can cause significant damage to the brain. Further, it makes the body vulnerable to a host of opportunistic infections – infections that would not normally affect a person with a healthy immune system (“AIDSmeds”, 2009). Many of these have significant impact on brain functioning.
1. In the early stages the disorder is characterized by minimal cognitive and motor impairments as shown by slowed information processing and slowed extremity movements. The patient can function on his own with minimal assistance such as reminders.
2. As the disease progresses, there is functional cognitive, affective and motor impairment. The patient misplaces things, faces difficulty in performing complex tasks and has problems with verbal memory and new learning. There may be motor dysfunctions like tremors, leg weakness and loss of balance. The patient may become ambulatory, but may be able to perform the basic activities of self-care.
3. With further neurodegeneration, the subcortical dementia begins to resemble global cortical dementia. At this point, there is deterioration of intellectual function, decision making capacity, delirium, hallucinations and loss of behavioural control. The patient cannot walk unassisted, there is considerable slowing of all cognitive faculties (including speech and reaction time), and there may be affective symptoms like apathy, irritability and social withdrawal.
4. The end stage, marking full progress of the syndrome, is characterized by a nearly vegetative state, with rudimentary levels of intellectual and social comprehension and bladder incontinence.
Schizophrenia: Schizophrenia affects approximately 1% of the population worldwide and is a chronic, severe psychiatric disorder. The onset of schizophrenia usually occurs around 18-25 years of age and is often preceded by premorbid behavioral deviations, such as social withdrawal and affective changes (Keshavan et al., 2005). Psychiatrist Emil Kraepelin, was the first to acknowledge psychiatric disorders from a biological perspective, and established the term dementia praecox. In 1911, the Swiss psychiatrist Paul Eugen Bleuler renamed dementia praecox as “the group of schizophrenias” and described it as a cluster of disorders rather than one coherent disease. With reference to prognosis, Crow (1980) classified two categories – type I and type II. Type I schizophrenia patients are those who present, often more acutely, with a predominantly positive symptom profile and who have a good response to neuroleptics or antipsychotics. In contrast, type II schizophrenia patients are those who have a more chronic illness, more frequent evidence of intellectual impairment and enlarged ventricular size and cortical atrophy as seen on CT or MRI scans, a poorer response to neuroleptics and predominantly negative symptoms. Type I category of patients possessed symptoms which are excess or distortion of normal mental functions like hearing voices, so these symptoms are called as positive symptoms. And Type II category patients possess symptoms which are loss or reduction of normal functioning like asocial behavior. These are called negative symptoms. Diagnostic Statistical Manual (DSM-IV-TR) accepts this classification. Of the two types, the negative symptoms are more difficult to evaluate because they may be influenced by a concurrent depression or a dull and un-stimulating environment, but they account for much of the morbidity (unhealthiness) associated with schizophrenia. The positive symptoms associated with better prognosis as compared to negative symptoms.
Positive Symptoms: The positive symptoms of schizophrenia include four "first-rank" or Schneiderian symptoms, named for a German psychiatrist who identified them in 1959 and other positive symptoms.
Ref: http://www.nios.ac.in/srsec328newE/328EL5.pdf
Dutta Roy,D.(2006). Development of picture drawing test to assess consciousness layers of tribal children of Tripura, Journal of the Indian Academy of Applied Psychology,Vol. 32, No. 1, 20-25



